Rob Beatty, MD FACEP
Every year, the influenza virus wreaks havoc on the world, and its arrival is anticipated by hoards of people, students, and healthcare workers getting their annual “flu shot.” Influenza is its own type of virus, and is composed of two specific genetically variable markers, labeled H and N. This virus becomes genetically prevalent based on what are known as antigenic shifts, which create different combinations of H and N, making the virus unique on an annual basis.
HN Variants
Sometimes, the HN variants are mild in nature. Other times, the HN variants are extremely contagious and potentially deadly, such as with the H1N1 outbreak a few years ago and also in 1918. The manufacturers of the influenza vaccine try to anticipate the correct H and N frequencies by combining a mixture of expected variants into their annual flu vaccine. This means that when we get our annual flu vaccinations, we are being given relative immunity for the most commonly expected types of flu for that season. Sometimes the prediction is right on. Sometimes it’s way off, and ineffective. In addition to the antigenic variance, there are two strains of influenza virus- A and B, which can also mutate through the course of a flu season or outbreak, and change their symptoms and effects on a community.

Influenza Virus Structure (above)
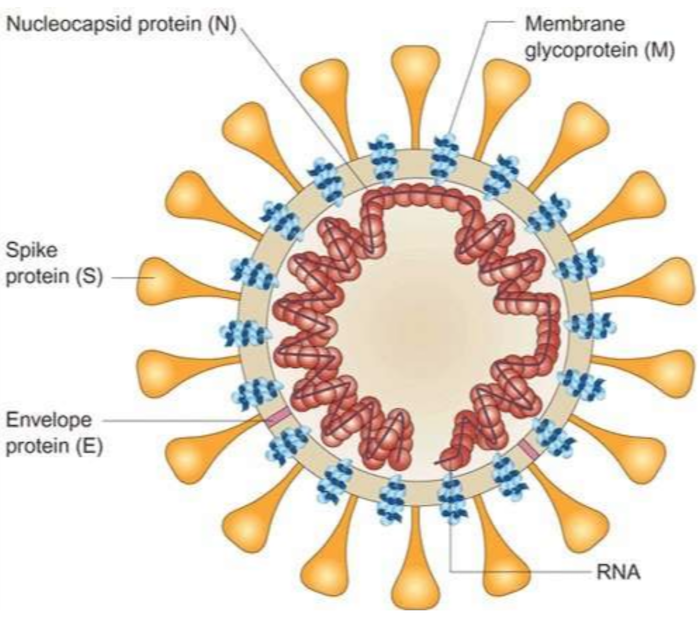
The coronavirus (above) is conceptually not much different from the influenza virus, but it is important to remember that it is its own type of virus altogether.
For perspective, it is important to remember that the common cold is most commonly caused by respiratory viruses like the coronavirus, which due to its structure is very easily spread person to person through droplets.
So what makes the novel coronavirus (COVID-19) so different?
To start, let’s discuss how viruses work, and what makes them unique to the cellular world. Unlike bacteria, which are their own living cellular organisms, viruses are specially designed microbiotic structures that are designed to enter cells and change the way they make things. Different cells in the human body are responsible for creating different products that the body uses for its combined functions. For example, brain cells create neuroproteins designed to aid neuronal conduction. Skin cells produce sebum for lubrication and protection, and lung cells produce secretions for mucous, which delivers impurities away from the alveoli, and prevents contamination into the bloodstream. These are just a few examples, and cells can produce hundreds of unique products.
Depending on the virus, and the type of cell it attacks, different body structures can be effected in different ways, and at times, simultaneously. When a virus has an “affinity” for a specific body tissue, its effects can be profound.
Virus Mutations
As we mentioned with the flu, viruses are known to mutate within a community as they encounter different cellular DNA among different species. Another good historical example of this concept can be seen with the bird flu, which caused a severe mutation of the influenza virus that was derived from chickens as the host, and caused a transmission to humans that was extremely severe. The novel coronavirus is thought to be derived from bats in the Wuhan territory in China. Novel is language for new or never-before-seen. This novel virus is believed be created by a natural mutation that altered the spike protein of coronavirus, making the virus extremely virulent against humans, and specially human lung tissue. This mutation converted the common cold bug into a super virus with lethal consequences greater than the basic coronavirus.
Genetic Predisposition
In addition to viral tissue targeting, there is a suggestion that certain genetic communities may be predisposed to varying degrees of disease severity. Research performed by Dr. Emma Hodcroft in Switzerland has documented this variance in presentation in European communities, suggesting that certain ancestral lineages (high tech talk for related people) are predisposed to getting very ill from COVID-19. As a result, this novel virus has a rapid spread between members of a population and a vastly variable effect on disease presentation, likely due to genetic factors in the host (us). The ease of transmission of novel coronavirus (COVID-19) is responsible for the high degree of concern for containing this virus, and in the great efforts we have taken to mitigate its spread.
Preventing the Spread of COVID-19
It is likely that you have heard the phrase “flatten the curve” being used frequently in the news and in scientific circles. The field of epidemiology focuses on the prevalence of a disease and its likelihood to infect a population. In addition, it considers the resources that are needed to prevent the spread of a disease in a certain population. In the case of COVID-19, the rapid spread is highly concerning, because as transmission occurs through droplets (water vapor and exhaled particles from an infected host), and the time to develop the disease averages 5 days, the potential for a population to become quickly consumed by the contagion is very high. The disease itself does not have a high mortality rate, but the rapid drain and overburdening of healthcare resources that can manage it is profound. So profound that it quickly overwhelms the capacity of healthcare delivery, crippling hospitals, filling hallways, exhausting ventilator and provider supply, eventually wiping out any meaningful ability to manage sick patients. Clearly, a bad scenario and one that would spell disaster for a population, or even the human population.
This rapid initial infection outbreak creates a sharp “spike” of infected people in a community. By mitigating the spread of the virus (through practices such as social distancing, public closures, mandatory PPE use, and other isolation strategies), the goal of mitigation is to slow the inevitable spread of the virus so that the public health resources can manage it, and continue to provide care to sick patients. This so called “flattening the curve” was adopted by China initially, and eventually by many other modernized nations. In the United States it led to the large swathe of closures, “lockdowns,” and other isolation techniques.

Origin of COVID-19
There are several theories regarding the actual origin of COVID-19. Some believe this virus may have originated in a laboratory in China. If an evil scientist were to design the perfect biological agent to destroy a population, that agent would need to meet three requirements:
- It would spread quickly by basic human transmission routes without a means of surveillance.
- Its disease would be rapidly progressive, highly lethal, and impossible to cure.
- It would be difficult to contain and track.
This is not suggesting that the coronavirus was part of a sinister plot to infect the world, but instead to put into context the traits that make COVID-19 such a scary global concern with potential epidemiological and national security concerns. In a more likely scenario, this is a bad virus that is the result of genetic adaption and mutation through many generations of species to species transmission.
COVID-19 Mortality
Much surrounding this outbreak and pandemic is that little is understood about the virus. This specific virus can be carried completely asymptomatically and transmitted without them knowing it, making the true number of “infected” people even higher, and unknown. The walking well who have the virus may never be sick enough to know they need testing, and if they were, they would likely dilute the true mortality of this infection to an even lower percentage. Based on data from mid May, 2020, the actual overall mortality of coronavirus is approximately 80,000 people in the United States. With an estimated US population of 328 million people, the overall mortality attributed to COVID-19 is .02%. As of mid-March 2020, the CDC has estimated that the total of number of deaths attributed to influenza is between 29,000 and 59,000 for the year 2020. By comparison, the overall mortality of common causes of death in the United States is as follows:
| Cardiovascular Disease | 647,457 |
| Cancer | 599,108 |
| Accidents | 169,936 |
| Chronic Lower Respiratory Diseases | 160,201 |
| Cerebrovascular Diseases | 146,383 |
| Alzheimer’s disease | 121,404 |
| Diabetes | 83,564 |
Source: National Vital Statistics Reports, Vol. 68, No. 9, June 24, 2019, CDC
It is likely that, as the final tally of mortality for 2020 is recorded, COVID-19 will surpass Diabetes as a common cause of death. Very sobering, with the exception of a few discrepancies in reporting that may be falsely elevating data. For example, in the city of New York, arguably the largest COVID-19 epicenter in the world, nearly all deaths are being diagnosed as COVID-19. This includes myocardial infarctions, strokes, cancer, and other common causes of mortality that are attributed to the virus instead of their actual and (more likely) cause. Conversely there is also variability in the diagnosis of common diseases that may actually be due to COVID-19 due to limited testing. While we may never know the true number of COVID-19 deaths, mitigation strategies put in place will likely cause an overall decline in mortality from the virus as time moves forward.
Then there’s the children mystery. For whatever reason, COVID-19 initially seemed to leave children largely unaffected, and pregnant mothers who tested positive for the virus were having babies who were testing negative, initially suggesting the virus did not cross the placenta, and does not impact fetal cells. Additional studies are beginning to demonstrate that there may be intrauterine transmission after all. To confound things even more, children are also now appearing with vascular inflammation and a Kawasaki-like syndrome as a result of this infection, causing even more confusion.
It is highly likely that the evolving disease presentation and changing clinical findings are the result of viral mutation. The latest estimates from mid-May 2020 suggest that the actual number of COVID-19 viral strains is around 14, with even more being likely. In fact, it is estimated that the majority of worldwide infections since mid-march are caused by the newest of these 14 strains. This has far- reaching implications for the pandemic because as the virus changes, its effects on different organ systems is impacted. Furthermore, this data was published while vaccination research based on prior known strains had previously begun, thwarting progress made to this point. These mutations make disease more variable, transmission more rapid, and also open the door to reinfections of those who had previously been infected.
The Viral Reaction of COVID-19
So there you have the current situation- a novel strain of a likely genetically targeted virus that is not well understood, transmitted globally, and causing death. While the mortality data may be unreliable, there is no doubt that public sentiment is led by fear of the unknown. People don’t handle panic well, and the media feeds on scenarios such as this to garner attention and viewers. Fact checking is a challenge because multiple sources are changing their information daily and, well, relying on the Chinese to provide us with accurate data is a challenge even with good news. In short, the hysteria surrounding COVID-19 may be well-founded, or may be a byproduct of emotional reactions generated by unfounded fear. Only time will tell. What we do know is that after a short 3 month time period, COVID-19 infections declined in China- if you trust their data. However, as China reopened their doors and businesses, a second wave of outbreaks has occurred.
This virus has led to an unprecedented reaction from the international community, resulting in closed borders, cruise ships being denied portage, and literally entire cities being placed on lockdown to avoid spreading of the virus. Similar to movies involving zombie apocalypse themes and other fictional disease themes. The truth is that the scientific community must assume the worst, and governments must, despite political and economic pressures, do what is right for the global community.
Perhaps more concerning about this “viral reaction” is the discovery of how woefully unprepared we are as a nation and a world. The US CDC has suggested that a 6 foot radius is ideal to avoid transmission of droplets from one person to another. Alternatively, wearing face masks can reduce the need for this spacing. However, the type of mask (surgical, N95, etc) has not been universally agreed upon by epidemiologists and public health authorities. The reality is that even if there was a consensus about the right type of mask, there aren’t enough in the world to safely protect everyone. While production efforts are increasing, it will be a long time before supply reaches demand. Also, the misuse and overuse of PPE will contribute to this shortage. Anyone who has seen a person driving their own car alone, wearing a mask and face shield can appreciate how good intentions can lead to cumulative misunderstanding.
Human Hygiene
Hand hygiene has also been recommended and while a shortage of soap may not be likely, hand sanitizer is also in short supply. These known limitations have rendered all guidance from the CDC effectively meaningless, and without a miracle production of face masks and hand sanitizer, the only “easy” solution to limit the spread of the virus is to quarantine people and keep them out of the public domain. Factories have closed. Food production facilities have been shuttered due to internal infections, and the food supply of our nation may be under threat. As we enter a phase of reopening, there is little consistency between state to state regarding what a cohesive plan will be, but it appears to be data-driven and appropriate for disease prevalence. The general public can only be locked away for so long before they yearn to be free, and as public sentiment against isolation and lockdown turns toward re-opening and a return to normalcy, it is likely that public health initiatives will fail in favor of commerce and economic recovery. After all, this is also an election year!
Self Isolation
Despite these clear limitations, we are still isolating high risk people who are symptomatic and require COVID-19 testing, which is also in short supply and with limited availability. The initial testing guidelines suggested that patients with a fever, AND a cough, AND a history of travel should be tested for COVID-19. Over time this has morphed to include patients with risk factors such as obesity, hypertension, immunocompromised states, and age over 65. Current guidelines also include screening for loss of taste, smell, chills, sweating, or general weakness. It will only be a matter of time before every possible symptom of any infection will meet a screening criteria, leading to the eventual need to either test everyone for COVID-19 or treat everyone as if they are infected.
COVID-19 Testing
Even if we decide testing is warranted, there is still differing consensus at the state and even local level about who should administer the test and where patients should wait for the results, which can take as long as 48 to 72 hours after the test is received. Rapid tests (45 minutes or less) are being developed, but their accuracy is in question, with reported sensitivities ranging from 45% to 85%. Even those being used in the White House at this time have a reported low sensitivity. These low-sensitivity tests are discouraging because the number of false negative patients in our community will continue to contribute to the disease transmission.
Then there’s the multi-billion dollar question: What is the utility of a positive test result? If a patient has a cough, fever, and they are 18 years old without any risk factors, they are very unlikely to experience major complications. So why do we test?
We know that the disease progression can be severe and that a certain percentage of patients, for whatever reason, will develop severe pulmonary disease. Recent data has suggested there is a tipping point between the mild symptoms and the severe pulmonary disease that causes high mortality rates. Overall, it should be noted that over 80% of all COVID-19 positive patients experience only a mild upper respiratory illness.
We also like to have answers, which make us feel better about our likely illness outcome and allow us to identify those who should be isolated. The bigger question we should ask is how do we test those who have already been infected, and will be become immune. Most human viruses we are are familiar with confer a life-long immunity. Measles, Mumps, Rubella, Chickenpox – to name a few – are usually a “one and done” infection, and vaccination leads to permanent immunity. It would be ideal if we could test for COVID-19 antibodies that confirm immunity exists. There has been much in the media and in national planning surrounding antibody testing as a possible means to navigate the pandemic. In a brief nutshell, acute exposure to a disease cause an initial spike of Immunoglbulin M (IgM) which can be seen by itself in the bloodstream for up to 10 days. The solo appearance of IgM implies an acute infection period exists. As the

immune system recognizes the virus and begins to create antibodies to treat it, there is a testable overlap between IgM and IgG in the blood. Is IgG begins to appear, IgM disappears, and IgG remains as the final proof of prior exposure.
With common human viruses, the presence of IgG defines immunity, meaning that a person who has IgG for a specific virus has previously been infected and can’t get infected again. We are learning that this is not the case with COVID-19, as people are testing positive for the virus again – with acute infections – weeks and months after initially getting the disease. This is very concerning because it suggests that there may not be any form of immunity to the virus, making attempts at production of a vaccine meaningless. The old saying that “there is no cure for the common cold” may apply.
It is possible that this virus could mutate or reappear in a similar fashion for years to come. It may never be eradicated.
Byproduct of COVID-19
Perhaps the most sobering thought is that our nation’s hospitals and emergency departments, known as safe havens for identification and treatment of disease, have become areas feared by our population, and avoided. While the data is not known, it is reasonable to postulate that more patients will die without seeking emergency or hospital care, and other disease mortality will increase. Cardiovascular deaths will rise, untreated and undiagnosed cancers will become more prevalent, and preventable severe illness from diabetes and other diseases will soar. Medical science may go backwards because people are afraid to see their own doctors, and the fear of COVID-19 may blunt the reality of other more common diseases.
Progressing Through COVID-19
As we progress into the mitigation phase of the disease, we must all realize that containment is no longer a possibility, and the virus will run its course in our communities and across the nation. As the phase implies, the best we can hope for at this time is to reduce the number of people who get this disease, and limit their transmission to others as a whole. Reopening will proceed with diligence and data as their driving forces, and it is likely that, as disease outbreaks continue to appear in pockets of the country, and a re-emergence of the disease becomes a possibility, we may resume the containment-mitigation process all over again, leading to more closures, and a reconfinement of our society.
We must each do our part to watch for signs and symptoms in ourselves, and avoid exposing each other when they present. Pandemics and epidemics are a natural part of disease transmission, and since the 20th century have mostly been viral in nature.
As we move into the next few months, we owe it to ourselves and each other to be vigilant, careful, and responsible with our bodies and exposures. COVID-19 may not be the global killer that we fear, but if transmission remains high, that could equate to more severe illnesses and deaths. The reality is that by controlling the disease exposure rate, and keeping total infection rates low, the total lives lost will equate to a very small and imperceptible fraction of that total number.
A healthcare providers, we are determined to diagnose and treat our patients, and we are used to a world and a healthcare system that supports us in this endeavor. As this pandemic continues, and this specific novel virus continues to evolve, our world, our economy, and our entire healthcare system, will evolve with it. These are truly amazing times to be alive, despite the devastation and tragedy we must experience. We at Provider Practice Essentials are proud to be with you as we all experience these extraordinary times and hope to one day have a cure for the common cold.