Alex Koo, MD
Dental Pain and related emergencies range anywhere from 0.4-10% of all emergency department (ED) visits and depend largely on your practice setting and environment.1 Many times, patients come to the emergency department seeking relief from pain and the inability to see a dentist in a timely manner. While most dental pain complaints do not require emergent dental treatment, understanding the more dangerous etiologies that sprout from dental disease is important. In addition, understanding dental diseases can help allay patient anxieties, pain, and fears.
Anatomy
Firstly, understanding teeth anatomy is helpful to identify affected teeth and location of disease. Deciduous teeth (primary teeth) are the teeth that first grow out during childhood. They amount to 20 teeth: 8 incisors, 4 canines, and 8 molars. Then, at about age 13, most of our primary teeth have been replaced by our permanent teeth, which amount to 32 teeth: 8 incisors, 4 canines, 8 premolars, and 12 molars. Four of these molars are also our “wisdom teeth” and a significant proportion of Americans have them removed. About 5 million of these third molars are removed every year in the United States.2
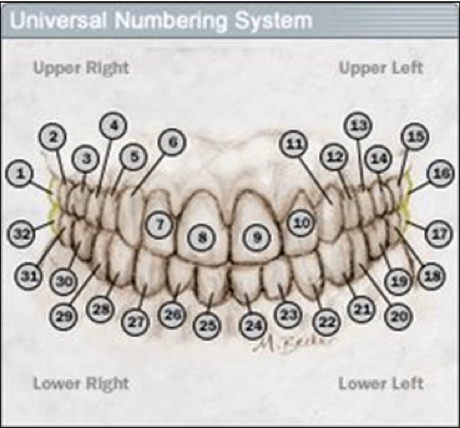
Numbering permanent teeth range from #1 to #32. #1 starts with a patient’s upper right molar/wisdom tooth going to #16 on the patient’s upper left molar. Then, starting at the #17 on the patient’s lower left molar to #32 of the patient’s lower right molar. Sometimes, patients may be missing a significant number of teeth and it may be easier to document teeth by their type and location (i.e. upper left incisor, right lower premolar etc.).
Finally, the anatomy of a tooth consists of the crown, which is the exposed portion of the tooth and the root, which is nestled in the gumline. Firstly, the tooth’s outermost layer is enamel, an insensate portion comprised of hydroxyapatite. Further inward, there is dentin, a yellow layer and finally the deepest layer is the pulp, which contains nerve and vascular supply. When there is significant intrusion of disease into the dentin or pulp, patients may experience tooth pain.
Pain Control
Pain control for dental complaints can be achieved with Acetaminophen and NSAIDs in combination. Typical regimens can be ibuprofen 400 mg every 6 hours with food and Acetaminophen 1000 mg every 8 hours. Many studies have demonstrated adequate pain control, similar to opiates with this regimen. However, if opiates must be used, careful use and the least amount for shortest course possible should be done. Other agents in dental pain as eugenol can be topically applied for anti-inflammatory and analgesic effects. Lastly, nerve blocks can be used to afford the patient temporary relief. This is outside the purview of this post, but examples would be suparperiosteal, inferior alveolar, mental, and infraorbital nerve blocks.
Concussed, Subluxed, and Avulsed Teeth
Teeth are like bones, tough, but still prone to fracture. Unlike bones however, teeth do not have the ability to regenerate. If a force hits a tooth, it can become “concussed”, “subluxed”, or completed “avulsed”. Concussion and subluxation will present with tooth pain or increased mobility, which can be tested with a tongue depressor. On physical, there may be some bleeding along the gingiva. Avulsed teeth are the complete loss of a tooth. If a tooth is avulsed, it may be reimplanted within 2-3 hours. Handle the tooth carefully by the crown, gently rinse with normal saline, and implant it. Do not scrub or roughly handle the root as the periodontal ligaments rest in the root and can be disrupted, leading to higher failure rates of reimplantation.
Splinting concussed, subluxed, or avulsed teeth can require some ingenuity. One can use commercial products as zinc oxide molding (i.e. CoePak) to be molded and splinting to the adjacent normal tooth. If no CoePak is available, using the metal nasal bridge of an oxygen mask as the splint and adhering the metal to the teeth with cyanoacrylate adhesive (i.e. Dermabond) can be used.
Tooth Fractures
Tooth fractures are classified by the Ellis system, which determine the depth of fracture. Ellis Class I fractures only affect the enamel and patients will not have pain. Ellis Class II fractures go into dentin, which will have exposed yellow, softer material. There may be some sensitivity to cold. Ellis Class III fractures go to the pulp, in which there may be exposed “pink” pulp and is very tender or sensitive. Treatment consists of creating a temporary protective coating on these fractures, which are commercially available as calcium sulphate paste (DenTemp, 3M Cavit), and calcium hydroxide paste (Dycal). Update the patient’s tetanus and have the patient follow-up with a dentist, ideally within 24 hours.
Atraumatic Dental Pain
Ludwig’s Angina (Emergent)
This is a rare, but emergent diagnosis in which odontogenic infections can progress into the lingual, submandibular, and parapharyngeal spaces. Typically, the infection of the second and third molars are niduses for spreading infection and patients present with trismus, sublingual swelling. If the swelling is severe enough, airway occlusion is also an emergent concern. Suspicion should guide providers to obtain imaging as CT head/neck with intravenous contrast for deep space swelling or fluid collections. For children, hematogenous spread of bacterial infection can lead to Ludwig’s angina.4 Treatment is airway securement/evaluation, source control with drainage (if an abscess is present, intravenous antibiotics, ENT consultation, and hospitalization.
Cavernous Sinus Thrombosis (Emergent)
Cavernous sinus thrombosis is another rare, but deadly disease that can start with maxillary odontogenic infections and spread into the cavernous sinus via the ophthalmic veins. The infection can cause infraorbital swelling, headache, CNVI palsies, and also progress to meningitis. Diagnosis with CT head with IV contrast may reveal irregular filling defects in the cavernous sinus and ophthalmic vein thickening. Treatment is with intravenous antibiotics, admission, and ENT consultation.
Dental Caries
Dental caries can occur due to slow breakdown of enamel over time. Bacteria, acids, and lack of saliva production (i.e. methamphetamine use) can contribute to dental caries. To prove just how prevalent “meth mouth” is, a 2015 study of 571 methamphetamine users with comprehensive dental examinations revealed that 97% of the participants had caries and 58% had significant tooth decay.5 Typically, pain starts as cold sensitivity with dentin involvement, but can progress to pulpitis. Treatment in the emergent setting is with antibiotics of penicillin VK 500 mg QID or Clindamycin 300 mg QID for 7-10 days. While this may help control the infection and progression of disease, the patient will need dental follow-up closely for source control and definitive management.
Alveolar osteitis
Alveolar osteitis is also known as “dry socket” and is a localized osteomyelitis of the bone. It occurs about 2-3 days after dental extraction and specifically for wisdom teeth, will occur about 2-5% of the time.2 It will present with pain and treatment includes saline irrigation of the socket, penicillin VK, and also packing the socket with iodoform.
Acute Necrotizing Ulcerative Gingivitis (ANUG)
ANUG is an infection of the gums and can present with the triad of 1) gingival pain/ulcers, 2) interdental gingival necrosis, and 3) gingival bleeding. It typically occurs in patients with suppressed immune systems as HIV or diabetes. Treatment includes localized antibiotic rinses as chlorhexidine 0.1% BID and metronidazole 500 mg TID.
References
- Tintinalli, Judith E. Cline, David, et al. Tintinalli’s Emergency Medicine Manual. New York: McGraw-Hill Medical, 2012.
- Avoidance of prophylactic extraction of third molars can prevent this public health hazard. (Am J Public Health. 2007; 97:1554–1559. doi:10.2105/AJPH. 2006.100271.
- Rosenberg H, Rosenberg H, Hickey M. Emergency management of a traumatic tooth avulsion. Ann Emerg Med. 2011 Apr;57(4):375–7.
- Lin H, O’Neill A, Cunningham M. “Ludwig’s Angina in the Pediatric Population”. Clinical Pediatrics. 2009; 48:583-587.
- Shetty, Vivek et al. Dental disease patterns in methamphetamine users. The Journal of the American Dental Association. 2015. 146 (12): 875 – 885.