Taking the Mystery out of the Squiggly Lines
Scott Biggs, PA-C
Today we are going to dive in to one of the topics that seems to intimidate people more than just about anything else in medicine – how to read an EKG. This skill is often causes fear and confusion. I assure you that it isn’t nearly as difficult as it seems. The key to reading EKG’s, as with any big project, is to divide the task up into smaller, more palatable bits and then work your way back to the big picture.
Labeling the EKG
When you are first handed an EKG, there are a few things that you need to look at straight away, before you even try to interpret it. First, you need to confirm that the name and date of birth on the EKG label matches your patient. Although a simple step, this is a common error that can lead to confusion later on. It can be very embarrassing to tell the wrong patient that they may have a heart condition! While you are at it, make sure that the date and time are current and correct. Interpreting and EKG from several months ago doesn’t do the patient any good right now!
Rate
Once you have confirmed the EKG you are looking at is for the correct patient, and is the most recent one, then you need to start interpreting the squiggly lines. While this seems like a daunting task, it really isn’t so bad when you break it down. First, let’s diagnose the rate and rhythm present on the EKG.
Most modern EKG machines will give you a box of information at the top of the paper with a bunch of numbers. Typically, the first number listed will be the heart rate. If that number is less than 60bpm, it is a bradycardic rate. More than 100bpm, then it’s a tachycardic rate. A normal rate is between 60 and 100 beats per minute. See, not so bad! But what if the machine doesn’t give you a rate? Well, there are several tricks you can use but I find the easiest one is to count.
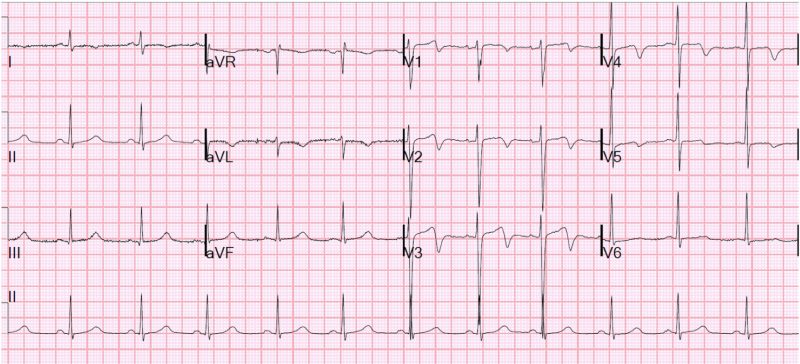
Typically an EKG captures 10 seconds of a cardiac rhythm. The very last line of an EKG is called the rhythm strip. So, if you count the number of beats in that 10 second strip and multiply that number by 6, you get the heart rate. In the picture above, that is 11 beats in 10 seconds, which works out to 66bpm. We are all taught how to read an EKG rate differently, but any method that works for you is good.
Rhythm
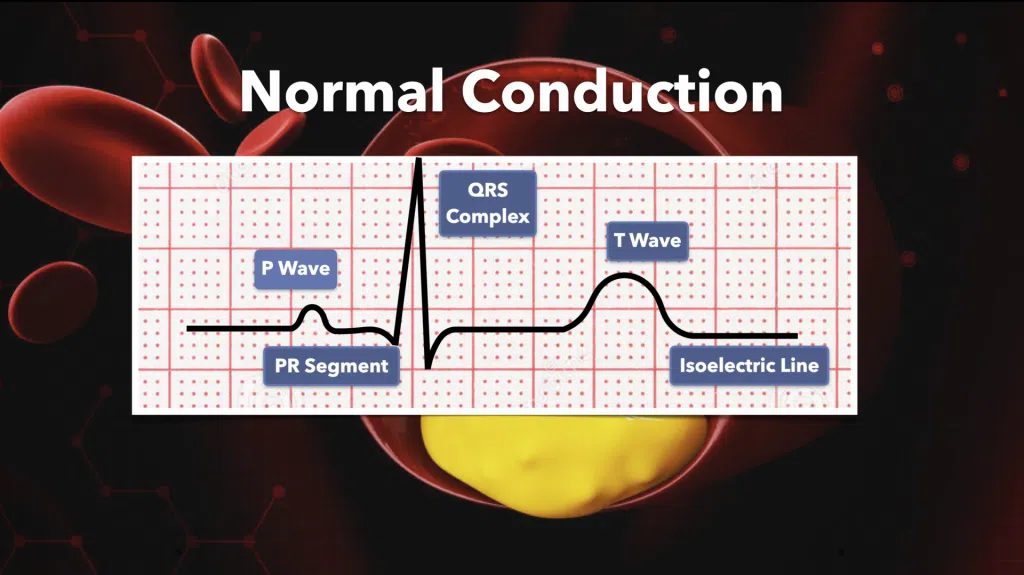
Now that we have the rate, let’s figure out the rhythm. If we continue to look at that rhythm strip, we will see that the QRS complexes come at a regular interval that steadily marches on across the page. There is a p-wave for every QRS complex, and a QRS complex for every p-wave. Also, the QRS complexes all have the same shape. This defines normal sinus rhythm. If the rhythm is not regular across the page, in other words some beats came closer together than others, them that would be an irregular rhythm. Irregular rhythms are not all bad, but you should be able to recognize the bad ones. This is a crucial part of knowing how to read an EKG.
Atrial Fibrillation
Atrial fibrillation is probably the most common, and concerning cause of irregular heart rhythms, and is one that every person who reads EKGs should be familiar with. In atrial fibrillation, the atria do not beat in a synchronized way, so p-waves are not present on the EKG. This disorganization causes current to pass through the AV node at different intervals, causing irregular contraction of the ventricles, and therefore irregular intervals between QRS complexes on the EKG. Atrial fibrillation has an “irregularly irregular” QRS pattern on an EKG.
Premature Contractions
PAC’s and PVC’s are other causes of irregular rhythms on EKGs. “PAC” stands for premature atrial contraction. These are cause by excited or irritated cells in the atria that cause an “early” contraction of the atria. This causes an early QRS complex. “PVC” stands for premature ventricular contraction. These occur when irritated ventricles cause early depolarization. These are not triggered by the atria. PVCs do not always translate into ventricular contraction, but they may. While PACs are usually benign, PVCs can be a sign that the heart is becoming increasingly irritated. This may warrant further investigation by an electrophysiologist.
Random, isolated PVCs are usually a benign condition. Also, PVCs may appear every other beat (bigeminy) or every third beat (trigeminy). However, when PVCs appear right after each other, they are called “couplets” and can be significant. Three PVCs in a row is the definition of non-sustained ventricular tachycardia. Episodes of bigeminy and trigemini should get your attention and are benign. However, episodes of non-sustained v-tach need to be investigated.
Intervals
The intervals we are talking about here is the interval between each small component of the cardiac cycle. Again, modern EKGs will have all of this information in the “numbers box” at the top of the page. Thankfully we don’t have to break out the calipers and measure these manually anymore! The important things to know here are what long intervals mean, and what you need to look for when you find them.
PR Interval
Let’s start with the PR interval. The PR interval correlates to the time it takes for the atria to depolarize and the electrical current to reach and travel through the AV node. A normal PR interval is less than 210 milliseconds in duration. A first degree AV block occurs when the PR interval is longer than 210ms. 1st degree AV block can be a completely benign finding, and is nothing to usually be too concerned over. However, a new 1st degree AV block may be due to drugs, medications, or electrolyte abnormalities. Knowing how to read an EKG and finding subtle changes he
PR intervals will also change for other kinds of heart blocks as well. 2nd degree heart blocks are classified in two different types. 2nd degree Type 1 heart block has a progressively lengthening PR interval until a QRS complex is dropped. This does not usually progress into an unstable rhythm and does not require inpatient evaluation. 2nd degree Type 2, however, is a serious finding that does require admission for further evaluation. It is classified as a steady PR interval with a randomly dropped QRS complex, often times in a set block suck as 2:1. 3rd degree heart block is also known as AV dissociation. Here, the AV node is completely blocked. P waves are no longer in rhythm with the QRS complexes. This will require hospital admission as well as placement of a pacemaker.
QRS Interval
Next, we will look at the QRS interval. The QRS interval represents depolarization of the ventricles, and is typically less than 120ms. Widening of the QRS complex and prolongation of the QRS interval is often associated with pathology. This could be due to a conduction block. A widened QRS, should be investigated if it is a new finding. Possible causes include drug toxicity, hyperkalemia, hypermagnesemia, WPW, and hypothermia.
QT Interval
Finally, we will look at the QT interval. The QT interval correlates to the time from the completion of the depolarization of the ventricles to the completion of the repolarization of the ventricles. This interval has received a lot of press lately as it seems that every medication known to man will cause a prolongation of the QT interval. A normal QT interval is less than 450ms, but varies by sex, age, and heart rate. Usually, prolonged QT intervals are not concerning until they get past 500ms. Often, prolonged QT intervals are caused by medication, which is why we must be careful when prescribing medications that could possibly affect the QT interval, as there can be an additive effect.
Injury Patterns
Now that we have established our patient’s heart rate, heart rhythm, and if they are experiencing any electrical conduction abnormalities, we can start looking at the “exciting” stuff. When most people look at EKGs, the first thing they think of is “Is my patient having a heart attack”. EKGs provide so much more information than that, but now is the time to look for patterns of injury.
When evaluating an EKG for injury pattern, the first place we must look is the ST segment. This portion of the EKG tracing relates to how electricity travels through the heart. This segment Is often elevated above – or depressed below – the isoelectric line. The T-P segment defines the isoelectric state of the cardiac cycle.

ST Elevation
Patients who are experiencing an acute MI often have ST elevation in leads associated with the area of the heart affected by the blockage. To diagnose a ST elevation MI (STEMI), there must be at least 1mm of ST elevation in two contiguous leads on the EKG. Prior to the acute MI, patients my show ST depression and/or T-wave inversion on EKG when they are experiencing chest pain. This shows that a portion of the heart is not receiving the amount of oxygen in requires to perform the required tasks.
ST elevation usually occurs in specific leads based on blood vessel anatomy. The location of the injury can identify which part of the heart is injured. Leads II, III, and aVf are the “inferior” leads and correlate to the right side of the heart and usually the right coronary artery. This can supplies the low pressure right side of the heart. Leads V1-V3 are the “anterior” or “septal” leads, and often correlate to a lesion in the left anterior descending coronary artery, also known as the “widow maker”. Leads V4-V6, as well as leads I and aVL, are the “lateral” leads. These are associated with injury to the circumflex artery that leads around the left side of the heart.

Lead aVR – The forgotten lead
This leaves us just with lead aVR. ST elevation in lead aVR may correlate to a high-grade lesion of the left main coronary artery right as it comes off of the aorta. This can be controversial, because there isn’t an associated second contiguous lead with aVR, so therefore cannot meet STEMI criteria. These patients often have the usual acute MI symptoms; chest pain, shortness of breath, diaphoresis, etc. And if they have ST elevation in aVR, they will likely have ST depression or T-wave inversion (reciprocal changes) in all of the other leads. Patients who present this way need emergent evaluation by cardiology, but technically are not having a STEMI by definition.
So now you know the basics of how to read an EKG. This truly is the basics, and there is so much more information that can be gleaned from all of those squiggly lines! But, that is for another day.
The slides in this presentation are taken from our
Advanced Practice Provider Clinical Skills and Procedure Workshop
Our classic 2-day workshop designed for ALL Advanced Practice Providers. Current identification and management of urgent and also emergent conditions you are most likely to miss. Procedures to match! Learn how to save a life in any practice setting. CERTAINLY A MUST HAVE live course experience. Friday and Saturday.
SAMPLE VIDEO FROM OUR LIVE COURSE: