Camilo Mohar, DO
A commonly used ultrasound technique is the Focused Assessment with Sonography in Trauma (FAST). This exam identifies intra-abdominal bleeding. With the advent of ultrasound, many procedures have been relinquished to just the history of medicine. Likewise, deep peritoneal lavage (DPL) is one of those procedures. DPL was classically performed on patients with abdominal trauma who were deemed too unstable for CT. By testing for blood in the peritoneum, positive studies identified patients who needed emergent laparotomy. As a result of the FAST exam, this procedure is now rarely performed. Ultrasound has taken its place in the assessment of the undifferentiated hypotension in a trauma patient and here we discuss how to perform a FAST exam, when it should be used, and its clinical significance.
Indication
The FAST exam can also be considered by many to be part of the primary survey when performing ATLS [1]. This would be performed after the airway, breathing, circulation, c-spine, disability, and exposure have also been evaluated and stabilized [2]. The primary reason for this exam is to identify patients who are in hemorrhagic shock due to abdominal trauma.
Do all trauma patients get a FAST exam? This is debatable. Most guidelines state that FAST should be performed if a trauma patient is hypotensive, and/or too unstable for CT. CT imaging is the preferred study for stable patients. This is partly due to ultrasound’s limitations in identifying traumatic injuries. Ultrasound can identify intra abdominal fluid, however it has poor specificity. Likewise, fluid can be blood or ascites. The amount of fluid needed to appear on a positive exam can also limit its utility. The minimum amount to produce a positive finding is generally two hundred mL of fluid [3]. Some experts recommend placing the patient in trendelenburg. This increases the amount of fluid collection in Morrison’s pouch and likewise makes interpretation easier.

Location and Relevant Normal Anatomy
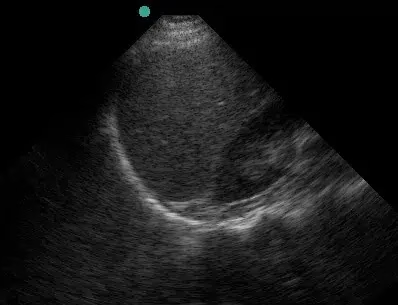
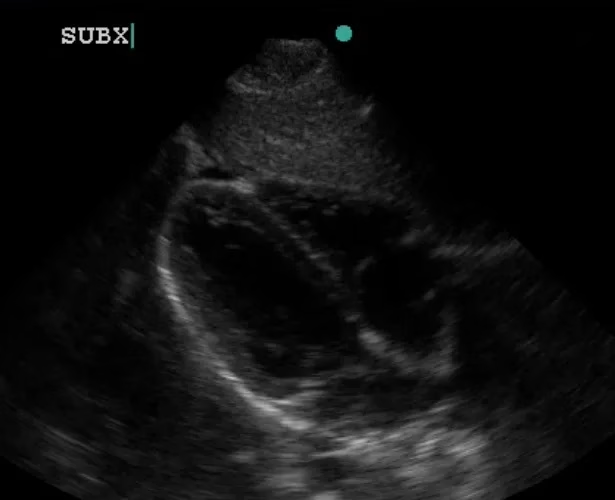
The FAST exam evaluates the abdomen for internal bleeding. Therefore, anatomic locations for probe placement include the A) right flank at Morrison’s pouch, B) the left flank at the splenorenal process, C) the suprapubic location above the bladder and D) the subxiphoid cardiac window .


Probe Selection and Position
This is an abdominal ultrasound and therefore requires the curvilinear array. If this probe is not available, a phase array can also be used.
Expected Positive Findings
The presence of dark (black) fluid in any of these areas is presumed to be blood until proven otherwise. Identification of a fluid space between organs takes a keen eye. Evidence of fluid around the bladder suggests peritoneal bleeding or bladder rupture. The subxiphoid view also provides insight into cardiac injury, and subsequent pericardial effusion. Any evidence of fluid in any of these four locations is a positive result. Laparotomy is indicated when a positive fast is performed in an unstable patient.



Complications
A negative FAST exam does not necessarily exclude internal bleeding as a cause of hypotension. Likewise, retroperitoneal bleeding cannot be identified with this technique.
Next Clinical Steps
Patients who have a positive FAST exam in an unstable setting should have blood sent, including type and cross for 2 to 4 units of blood. If the patient is in hemorrhagic shock, type O-negative blood can also be given empirically. This also provides volume for resuscitation and oxygen carrying capacity. Clinical judgement by a surgeon is necessary to identify the need for emergent laparotomy in these cases. Likewise, clinical judgement is necessary in cases where exam findings are not clear. An example of an equivocal study would be finding an unclear fluid collection (commonly between the kidneys and liver and/or spleen).
Additional Information and Tips
The clinical significance of a positive ultrasound has profound implications when applied to an undifferentiated hypotensive trauma patient. Several guidelines recommend subsequent laparotomy as the next step. Many trauma centers will have different providers tasked in performing such an assessment, and thus it is important to familiarize oneself with the exam, how to perform, and interpret it. The FAST exam has had indication creep in emergency medicine in evaluating other surgical emergencies. It points to the ease in assessing the presence of intra abdominal fluid in other emergencies such as ruptured ectopic, or ruptured
aorta [4].
Any cause of intra-abdominal bleeding can be evaluated with a FAST exam. An example can include suspected ruptured ectopic pregnancy. This can also be empirically suspected in patients without trauma, who have a positive HCG, and free fluid in the abdomen with sudden severe pain. This is especially helpful in patients who are hypotensive.
Stay tuned for other upcoming ultrasound posts, as we learn the different applications and techniques of ultrasonography in the ED in aiding our assessments of patients.
References
- https://www.ebmedicine.net/topics.php?paction=showTopicSeg&topic_id=252&seg_id=4
861 - https://en.wikipedia.org/wiki/Advanced_trauma_life_support
- https://www.ncbi.nlm.nih.gov/books/NBK470479/
- https://www.ebmedicine.net/topics/imaging/emergency-bedside-ultrasound
If you found this interesting and educational, you’ll LOVE our live and online learning programs!