Bunnany Chhun Pekar, PhD, CRNA, AGACNP
The purpose of this blog is to discuss some of the more common pulmonary disease findings. Please refer to my previous blog for a discussion on how to perform a complete pulmonary physical examination.
Before we begin, what does the term “clinical findings” mean?
Let us start with differentiating the difference between signs and symptoms.
According to King (1968), symptoms are manifestations that are apparent only to the patient, while signs are what the provider perceives. Typically, if the symptom is severe enough, such as shortness of breath, the patient will seek care. The symptom for which they come in for is referred to as the “chief complaint”. A sign is the objective evidence of the disease such as low oxygen saturation and presence of expiratory wheezing on auscultation. Likewise, the “clinical findings” would be a compilation of the symptoms and signs perceived by patient and provider. With a complete physical exam, laboratory findings, and history, this may point to a diagnosis for the reason of the chief complaint.
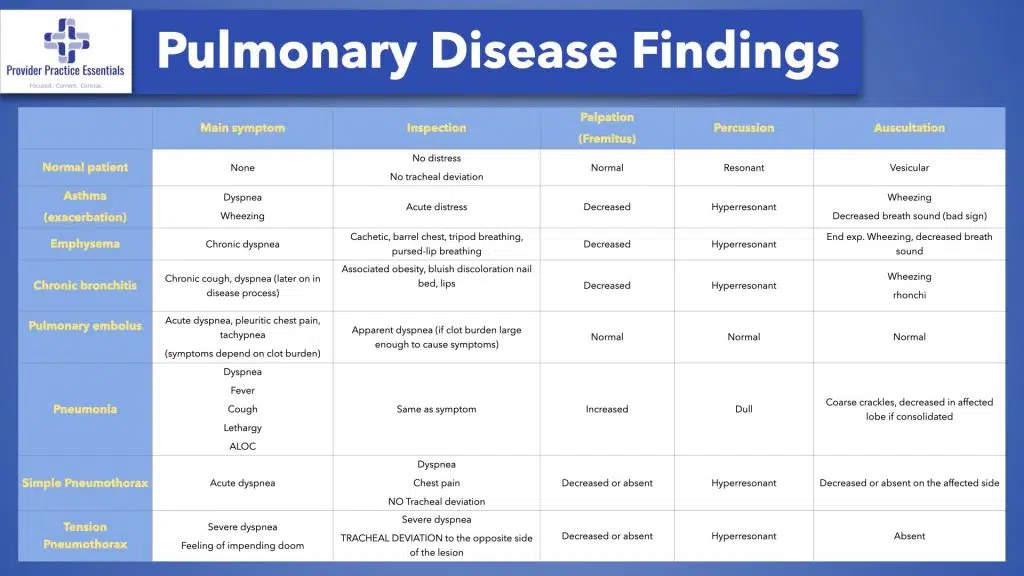
Recall that a complete pulmonary examination involves four basic components: inspection, percussion, palpation, and finally auscultation.
Common Conditions
Below are the seven common pulmonary diseases and their findings that you will encounter in practice placed in a table format. The four components of the pulmonary exam and the most likely presenting symptom(s) are also listed for each disease. In most cases, the way a patient presents and the findings from each component of the pulmonary exam also depends on how severe their disease is at that time. Therefore, as an example, a patient with mild asthma would have a normal pulmonary exam. However, a patient with an exacerbation or in status asthmaticus would present very different with different pulmonary exam findings. Likewise, some pulmonary disease such as a small pneumothorax or a small peripheral PE in healthy individuals may not have any pulmonary symptoms with normal pulmonary findings but maybe discovered incidentally through imaging.
Some Clinical Pearls That I Have Gained Over The Years
1) The side that moves less is also the side with the disease.
2) Tracheal deviation is a result of unequal intrathoracic pressure within the thoracic cavity. The trachea will deviate away from the lung affected by large amount of air, fluid and towards the lung that is consolidated or the side with the pneumonectomy.
Some symptoms may have pulmonary manifestation but have extrapulmonary cause(s). Likewise, a common example is cough. This may be related to GERD, especially if the cough occurs at night (reflux?) or associated heartburn. Another example is dyspnea which certainly has pulmonary manifestation but the etiology is numerous (hematological, cardiac, psychological, poor conditioning). A thorough history along with a complete physical examination may also point to the etiology.
COPD
Lastly, I would like to review a common pulmonary disease that you will definitely encounter in practice: COPD.
COPD is cluster of disease that includes chronic bronchitis, emphysema, recurrent asthma, and also bronchiectasis. Chronic bronchitis and emphysema are usually found together and have similar symptoms such as shortness of breath but they are two different chronic lung diseases. The primary cause of both of these diseases is smoking. However, some patients who developed emphysema are non-smokers and were not exposed to daily second-hand smoking but they have an alpha-1 anti-trypsin deficiency. Likewise, a patient may develop chronic bronchitis due to recurrent lung infections and is a life-long nonsmoker.
Emphysema
Patients with emphysema experience difficulty with gas exchange (carbon dioxide for oxygen) because of the destruction of the alveoli. These air sacs expand with resultant air trapping. The patient’s main symptom is shortness of breath, first with activity but as the disease progresses due to further destruction of alveoli, symptom will occur at rest. The findings from an arterial blood gas would therefore demonstrate hypoxemia, carbon dioxide retention, and elevated bicarbonate, which keeps the arterial blood pH normal. Patients with chronic bronchitis also tend to experience excessive mucus production and airway inflammation. The airways become blocked, causing shortness of breath, phlegm production, wheezing, and chest pain. It is characterized by a chronic cough that lasts for two months or more per year for more than two years
In differentiating between the two diseases, obtaining a complete history, symptom, and also performing a complete pulmonary exam may help point you to the diagnosis and subsequent treatment.
Examine the Lungs
As I mentioned in my last blog, physical examination, along with a thorough history is such an important tool in identifying the patient’s problem. In a study of patients admitted via the emergency department, 80% were diagnosed correctly based on history, physical examination, and basic laboratory testing alone, demonstrating that going back to the basics may also mitigate unnecessary tests and undue financial burdens on the healthcare system and patients.
Medscape (2014) conducted a reader poll and found that 75% of providers nearly always or often perform physical exams on their patients. However, the remaining 25% reported that they only sometimes perform physical exams on their patients. Likewise, reaching a diagnosis based on physical exam alone, only 50% of providers reported that they were somewhat confident in their skill. Thus, it is not surprising that 67% of those polled reported that diagnostic imaging and other tests supersede physical exam in making a diagnosis. However, it is encouraging that almost all providers who commented said that the physical exam is the art of medicine and should be performed in order to direct the diagnostic workup.
Diagnostic testing should be a complementary tool to the complete physical examination to aid in the diagnosis. Sometimes the patient may not be able to completely describe their symptoms but as a skilled observer, we can discern what the patient cannot. We can look, palpate, percuss, and auscultate to help us make the diagnosis.
References:
Asif, T., Mohiuddin, A., Hasan, B., & Pauly, R. R. (2017). Importance of thorough physical examination: a lost art. Cureus, 9(5), e1212. https://doi.org/10.7759/cureus.1212
Carr, S. (2020). Reexamining the physical exam. Retrieved from https://www.improvediagnosis.org/improvedx-january-2020/reexamining-the-physical-exam/
Elder, A.T. et al. (2017). The value of the physical examination in clinical practice: an international survey. Clin Med. DOI: https://doi.org/10.7861/clinmedicine.17-6-490
King, L. (1968). Signs and symptoms. JAMA. 1968;206(5):1063-1065. doi:10.1001/jama.1968.03150050051011
Max, J. (2009). The lost art of the physical exam. Retrieved from https://medicine.yale.edu/news/yale-medicine-magazine/the-lost-art-of-the-physical-exam/
Medscape (2014). Reader poll: the physical exam versus diagnostic test. Retrieved from Reader Poll: The Physical Exam vs Diagnostic Tests (medscape.com)
Mugambi, M. (2021). Chronic bronchitis versus emphysema: what’s the difference? Retrieved from https://www.mycopdteam.com/resources/chronic-bronchitis-vs-emphysema-whats-the-difference
Murher, J. (n.d). The importance of the physical exam in diagnosis. Retrieved from https://www.nursingcenter.com/ce_articleprint?an=00006205-201404000-00006
Stanford Medicine 25. (2021). Pulmonary exam: percussion & inspection. Retrieved from https://stanfordmedicine25.stanford.edu/the25/pulmonary.html
UC San Diego School of Medicine. (2018). Practical guide to clinical medicine: the lung exam. Retrieved from https://meded.ucsd.edu/clinicalmed/lung.html
OB Gyn key. (2016). Extra pulmonary diseases with pulmonary manifestations. Retrieved from https://obgynkey.com/extrapulmonary-diseases-with-pulmonary-manifestations/