Bunnany Chhun Pekar, PhD, CRNA, AGACNP
Question of the day:
What is the most commonly practiced part of the pulmonary physical examination?
The goal of this discussion is to review the components of a thorough pulmonary physical examination. We will also discuss if the performance of a physical examination is necessary. Advances in technology can aid in making the diagnosis quicker.

Lung Anatomy
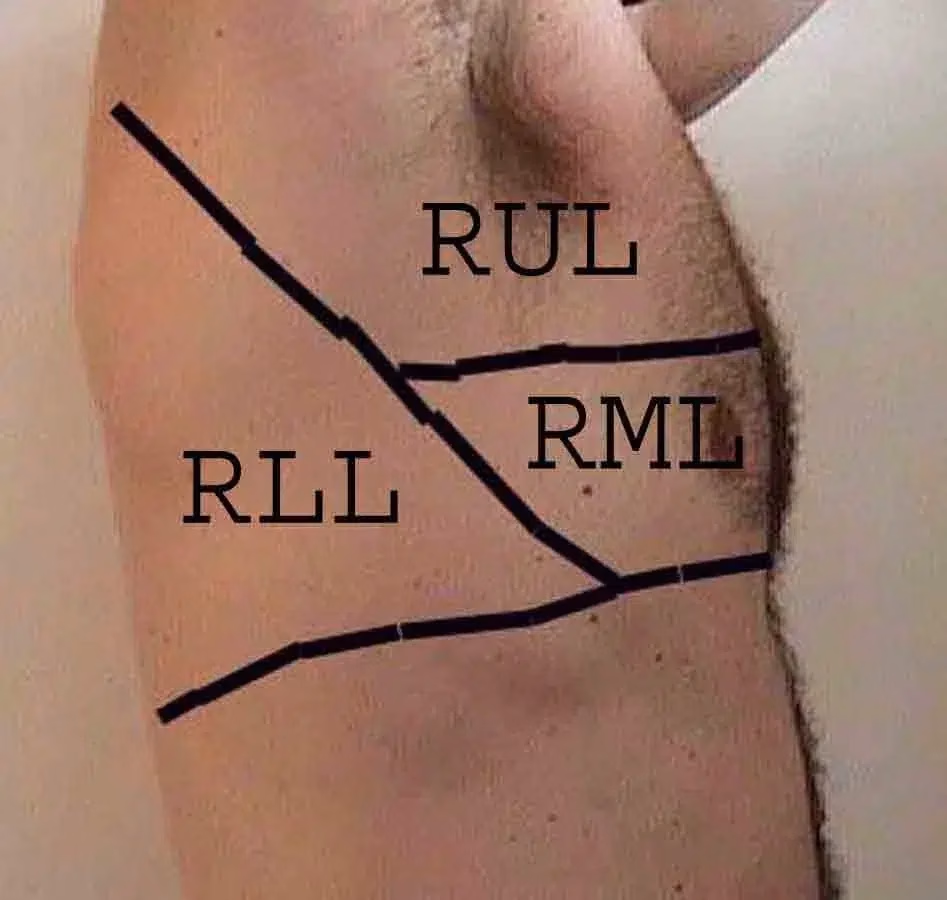
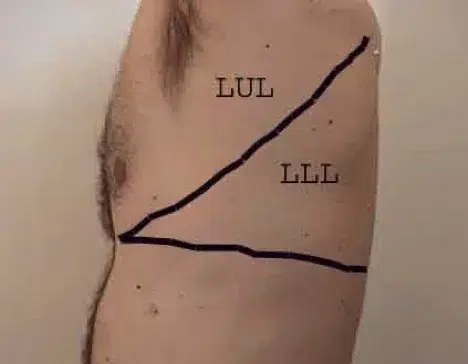
The diagrams below help you visualize which lobes you are evaluating. The right and left lungs are about the same size. The right lung has 3 lobes (upper, middle, and lower lobes). There are 2 lobes in the left lung (upper and lower). The left upper lobe essentially takes over the entire anterior hemithorax. The left lower lobe occupies 2/3 of the posterior thorax. There is also a lingula portion of the left lobe – which equates to the “middle” lobe of the left lung. The precise location of each of the lobes may not be appreciated on the physical exam, thus, these diagrams help you “visualize” which lobe you are examining.




The complete pulmonary examination
A thorough pulmonary examination involves four basic components: inspection, percussion, palpation, and auscultation. Let’s review each part of the complete exam.
Inspection
A large amount of clinical information can be obtained by simply observing the patient and also seeing how they are breathing. This is an often forgotten and basic part of the pulmonary physical examination. It is important to pay attention to:
- The patient’s general comfort
- Use of accessory muscles, pursed-lip breathing
- Patient’s color, especially around the lips
- Positioning of comfort (are they resting their hands on the knees and leaning forward to breath – a position known as tripoding?
- Ability to speak in complete sentences with breathing
- Audible noise that can be heard with the “naked ear” – where is the audible noise coming from (upper versus lower airway)
- Abdominal movement during inspiration (is it paradoxical with the thorax?)
What is the appearance of chest wall/spine? Take note of any of the following:
- Pectus excavatum
- Pectus carinatum
- Flail chest
- Scoliosis
- Kyphosis
It is important to note any extra pulmonary findings such as color or clubbing of nail beds
Percussion
This maneuver involves the provider placing the last 2 phalanges of their right or left middle finger and then tapping it with the opposite middle finger 2-3 times. Have the patient sit down and cross their arms to open up the chest. Tap along the posterior thorax between the vertebral column and the spine. This location is called the “alley for percussion.”

Percussion during the pulmonary physical examination causes a resonant note because the lungs are filled with air. This is the expected normal finding. The idea here is to percuss down the alley and repeat on the opposite hemithorax. A dull percussion in the thorax is an abnormal finding. However, dullness to percussion over organs such as the liver or heart is also normal.
It is important to also remember the “5-7-9 rule.” This is the upper border of the liver where you will encounter dullness with percussion:
– 5th intercostal space in the midclavicular line
– 7th intercostal space in the midaxillary line
– 9th intercostal space in the scapular line (approx. at the inferior border of the scapula)
Palpation
The examiner should also palpate the patient’s posterior thorax. To perform this, the examiner stands behind the patient facing their back. Both hands are placed on the patient’s back with thumbs pointed towards the spine. The patient is then asked to take a deep breath and hand movement is observed. The examiner’s hand should lift symmetrically outward when the patient takes a deep breath.


Don’t forget to also assess for tactile fremitus by asking the patient to say “ninety-nine” as you place the ulnar aspect of your hands firmly along both sides of the alley of percussion. The bony part of your hands is sensitive to detecting these vibrations. Repeat until you have covered the entire posterior thorax. Fremitus is also a normal finding as the lungs transmit a palpable vibratory sensation to the chest wall.
Auscultation
You are correct if you said that auscultation is the most practiced pulmonary examination.
To perform auscultation, the patient is asked to take slow deep breaths in and out through their mouth. Likewise, this allows for movement of greater volumes of air with each breath, increasing the duration and intensity of each breath. This also enables detection of any abnormal breath sounds that might be present. It may be helpful to ask the patient to cough a few times prior to auscultation to rid of any secretions or open atelectatic areas in the lower lobes that may obscure accurate assessment of breath sounds.
The pictures below will help identify which lobe is being auscultated during the exam. The right and left lower lobes are in the posterior aspect of the thorax.
When auscultating the lungs, it is important to listen to one side and then move to the same level on the opposite thorax so that you have a basis for comparison. The patient should sit upright. Alternatively, if they are unable to, they should lay on their side. In some cases, you are only are able to perform a limited exam by only being able to listen to the right upper and middle lobes and left upper lobe due to patient factors.
Sounds Have Meaning
In a healthy person who is breathing through their mouth at normal tidal volume, a normal auscultative finding is soft inspiratory sound with little expiratory noise. These so-called “vesicular breath sounds” are normal.
When performing auscultation, assess for egophany. Ask the patient to say “ee” as you are listening to them. A normal finding would produce a muffled “ee”. When the “ee” sounds like an “aa”, that is call egophany, an abnormal finding.
Also, assess for whisper pectoriloquy. Have the patient say “ninety-nine” softly. If it sounds louder in certain areas during auscultation, that is an abnormal finding.
Sometimes, the patient may complain of symptoms that occur only during activity, such as dyspnea on exertion. A dynamic lung examination may reveal whether the cause is pulmonary or cardiac in origin. Ask the patient to walk and assess for distance, ability to carry conversation (and how much), and gait, while observing pulse oximetry readings. This may also help quantify exercise tolerance and help in determining symptom/severity and aid in delineating possible problems. It may also help to determine which test to order based on those findings.
Examination and Testing
How often are all four components of the pulmonary physical examination used in actual clinical practice? It really depends on the care setting, severity of the presenting symptom, and also the patient’s body habitus. In an urgent care, ED, ICU, or other inpatient settings, the likelihood of employing all four of these components is very small because of these factors. As an intensive care NP and a CRNA, palpation and percussion of the thorax are not routine in my practice. However, inspection, auscultation, and focused palpation are the staples of routine patient care. However, the most information about a patient’s wellbeing is obtained through inspection.
Are clinicians still performing a thorough physical examination? Also, what is the role of diagnostic testing when making the diagnosis? In a survey of 2,684 practicing clinicians in the medical ward across multiple countries, 70% felt that physical examination was ‘almost always valuable’; whereas, 31% patients said that their provider never demonstrated use of the physical examination to them. 66% of trainees also felt that they were never observed by a provider when performing a physical examination on patients.
Summary
The physical examination, along with a thorough history is such an important tool in identifying the patient’s problem. This also applies to numerous clinical conditions that may not present as pulmonary complaints. In fact, in a study of patients admitted through the emergency department, 80% were diagnosed correctly based on history, physical examination, and basic laboratory testing. This data also suggests that going back to the basics may mitigate unnecessary tests and undue financial burdens on the healthcare system and patients.
In the upcoming second part of this topic, I will also explore physical exam findings of common pulmonary disease along with a discussion of the why diagnostic testing has been favored over physical examination.
References:
Asif, T., Mohiuddin, A., Hasan, B., & Pauly, R. R. (2017). Importance of thorough physical examination: a lost art. Cureus, 9(5), e1212. https://doi.org/10.7759/cureus.1212
Carr, S. (2020). Reexamining the physical exam. Retrieved from https://www.improvediagnosis.org/improvedx-january-2020/reexamining-the-physical-exam/
Elder, A.T. et al. (2017). The value of the physical examination in clinical practice: an international survey. Clin Med. DOI: https://doi.org/10.7861/clinmedicine.17-6-490
Max, J. (2009). The lost art of the physical exam. Retrieved from https://medicine.yale.edu/news/yale-medicine-magazine/the-lost-art-of-the-physical-exam/
Murher, J. (n.d). The importance of the physical exam in diagnosis. Retrieved from https://www.nursingcenter.com/ce_articleprint?an=00006205-201404000-00006
Stanford Medicine 25. (2021). Pulmonary exam: percussion & inspection. Retrieved from https://stanfordmedicine25.stanford.edu/the25/pulmonary.html
UC San Diego School of Medicine. (2018). Practical guide to clinical medicine: the lung exam. Retrieved from https://meded.ucsd.edu/clinicalmed/lung.html
Was this article helpful?
Check out our hands-on clinical skills and procedure workshop – designed specially for Nurse Practitioners and Physician Assistants!