Melissa Cody, ARNP
The chest radiograph (CXR) is by far the most commonly ordered radiographic exam. This is because it can give the clinician quick and easy insight into what may be ailing their patient. Most practice sites are lucky enough to have immediate access to a radiologist’s interpretation – but what if you don’t? What if the radiologist misses an anomaly? It is prudent for all providers to have a basic understanding of CXR interpretation.
To successfully evaluate a CXR you must take a systematic approach and understand basic anatomical findings. Let’s get started!
There are 3 ways to order a CXR:
PA (posterior-anterior) – Film is shot from back to front
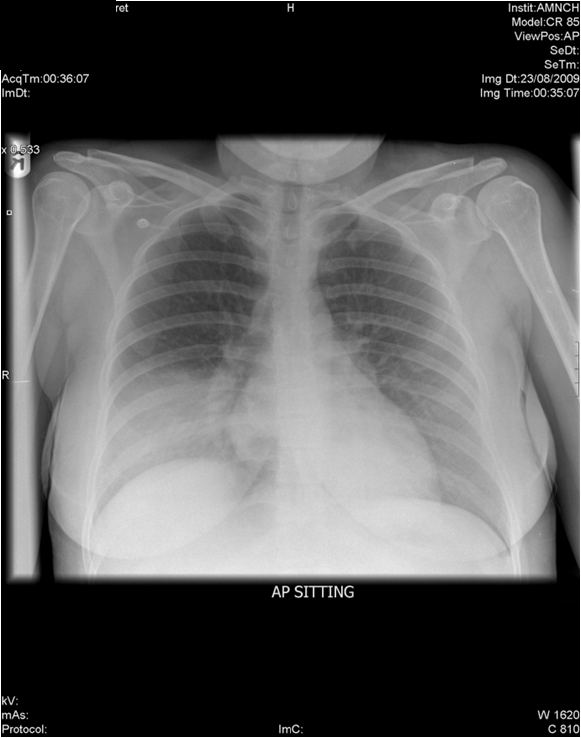
AP (anterior-posterior) – Film is shot front to back (typically ordered for inpatients)
PA/LAT (2 views: PA as above and lateral view)
In most outpatient centers you will be ordering a PA and Lateral view. Your patient will be set up with their front chest against the radiographic plate and the XR will be shot from their back. A lateral view is also helpful for assessment of the retrocardiac space.
My practice is in the ICU so I am ordering AP views 99.9% of the time. This view is useful for non-mobile or critically ill patients. The radiographic board can be slid in behind the patient and XR shot from the front. It is important to note that this view will artificially show increased magnification of the heart.
How to Interpret a Chest Radiograph
Interpreting a chest radiograph doesn’t have to be hard! Now that you have ordered the correct view, how do you interpret your film? Let’s review basic anatomy on the CXR. I typically refer my students to the picture below. It has an easy to visualize display of what you should expect to see on a ‘normal’ CXR.
There are many variations of this on the internet and I encourage you to go look at more pictures than what I can show you in the introduction.
Therefore, I can say with 100% certainty that the only way you will become comfortable interpreting CXRs is through repetition!

RIPP It!
Now that you feel more comfortable with the basic anatomy of the CXR that you’re viewing, what’s next? R.I.P is the first acronym I use for chest X-Ray interpretation. This will help you to assess the quality of the CXR. This time R.I.P will stand for Rotation Inspiration Penetration. I have also personally been taught to add an additional P to make it R.I.P.P. This second ‘P’ will stand for Prior.
- Rotation → Is the spinous process at the midpoint between the medial ends of the clavicles?
- Inspiration → Can I see 5-7 anterior ribs while counting down the midclavicular line?
- Penetration → Can you see the spine visible behind the heart?
- Prior → What variances do I see when comparing this new film to a prior one?
Applying the RIPP method will help to make chest x-ray interpretation easier and more clear.
ABCDE Method For Reading a Chest Radiograph
Next will be a systematic approach for chest x-ray interpretation. I like to use the ABCDE method:
- Airway: trachea, carina, bronchi and hilar structures.
- Breathing: lungs and pleura.
- Cardiac: heart size and borders.
- Diaphragm: including assessment of costophrenic angles.
- Everything else: mediastinal contours, bones, soft tissues, tubes, valves, pacemakers and also review areas.
As you use this approach, it will be easy to get stuck or stop midway through because you found an abnormality. Don’t get caught in this trap! You may have found that large right sided pleural effusion…woohoo! But did you notice that their right clavicle was also broken? Are there broken ribs? Perhaps this is a traumatic hemothorax vs. parapneumonic or CHF effusion. Point is, do not stop going through the ENTIRE approach because you found something, finish out the entire acronym. Remember when when chest x-ray interpretation uses a standard process, your differential diagnosis remains broad.
AIRWAY
Trachea → When evaluating the trachea you want to make sure that it is centrally located. If the trachea appears deviated to the right or left this is considered an anomaly (remember the normal anatomy from above?). Make note of this deviation before moving one with your assessment, DO NOT deviate from your systematic approach. You have already reviewed the quality of your film so you may also note if this deviation could be related to rotation of the film.
Carina and Bronchi: The carina is the point where the trachea divides into the right and left bronchi. The right mainstem bronchi is where you are more likely to find foreign objects or the tip of an inappropriately placed endotracheal tube. The reason for this is simply that the right mainstem is wider, slightly anterior and more vertically situated vs. the left mainstem.
Hilar structures: The left and right hilar regions should be roughly the same size. This region is also where the descending pulmonary artery intersects the superior pulmonary vein.
BREATHING
Lungs: This is a large area to review and there are a number of ways to do it. Two of the most common approaches are to break each lung into 3 equal zones or to use the zig-zag method. Either of these methods are appropriate. The point of each method is to inspect the bilateral lungs in relation to each other at the same points within the chest.
3 Zone Method
I will compare my right upper zone to my left upper zone. Are there abnormalities (consolidation, lack of airmarkings, symmetry, opacifications, GGO, ect…). Next I move on to the right middle zone vs. left middle zone. Finally the right lower zone vs. left lower zone. Remember: DO NOT stop because you found an abnormality, keep working the acronym.
ZigZag or Lawnmower Method
This is the same concept as the 3-zone method but with small sweeps bilaterally. I personally like this one, because my ADHD brain needs to have a tighter focus 🙂 That being said, find which one you like and STICK WITH IT!!! Pleura → The pleura should not be visible in a typical CXR. To inspect the pleura, inspect the borders of each lung to ensure that the lung markings extend all the way to the chest wall. Abnormalities include pneumothorax, hydropneumothorax, and also pleural thickening.
Let’s use what we’ve learned so far:

R.I.P.P → Rotation – none, Inspiration – good (8 ribs visible before diaphragm), Penetration – spinous process and vertebrae are well visualized, Prior – no prior films. ABCDE – Airway → Trachea is deviated to the left, carina and left bronchus noted but right bronchus not detected. Hilar structures obscured. Breathing → as I move from right lung to left I am noting an absence of lung markings in the right lateral lung. The pleura does not extend to the right lateral wall. We would continue through CDE for a full assessment. However, given what we’ve learned thus far, what is this problem here? If you said tension pneumothorax, then you were correct! You have a large right-sided pneumothorax that has also caused tracheal deviation. Now let’s continue.
Cardiac
The heart width should be less than half the width of the thorax at its largest point. If the heart is larger than this, the patient has cardiomegaly. The cardiac border should include the superior vena cava, right atrium, inferior vena cava, aortic knot, left pulmonary artery, left atrial appendage, and also the left ventricle.

Diaphragm
Typically the right hemidiaphragm will be higher than the left due to the location of the liver. Often under the left hemidiaphragm you may see a gastric bubble due to the presence of the stomach. The right diaphragm should also be indistinguishable from the liver. If you see increased lucency under the diaphragm then you should think pneumoperitoneum. This finding should be followed by CT of the Abdomen to assess for bowel perforation and source.
Along with the diaphragm, the clinician should also be making note of the costophrenic angles. They should be sharp bilaterally and are formed from the dome of each hemidiaphragm and lateral chest wall. The loss of a costophrenic angle (blunting) also often indicates the presence of fluid or consolidation. There can also be flattening of the diaphragms with costophrenic blunting. This alone with hyperinflation (think back to R.I.P) is an indicator of emphysematous changes (COPD). In the two images above note the hyperinflation, blunting of the costophrenic angles and especially the flattened diaphragms. This is a very ‘classic’ example of COPD:

Everything Else
Mediastinal Contours: The mediastinum contains the great vessels, the heart and lymphoid tissue.
Aortic Knuckle/Knot/Knob: lateral edge of the aorta as it arches back of the left main bronchus. Reduced definition of the aortic knuckle contours can occur with an aneurysm
Aortopulmonary Window: The space between the arch of the aorta and the pulmonary arteries. This space can be lost with mediastinal lymphadenopathy (reactive, malignancy)
Bones: Top to bottom and right to left. Inspect the visible skeletal structure for variations. This again needs to be systematic in it’s approach. Note any fractures, lesions, absences.
Soft Tissues: Look at all the soft tissue for abnormalities. Once again, I like the top to bottom, left to right approach. Are there hematomas? Subcutaneous emphysema? Absence of breast tissue unilaterally?
Tubes, Valves and Pacemakers: Ensure proper placement of any tubes or lines. Does your NG tube course below the level of the diaphragm? Does your central line terminate at the correct location?
Artificial Heart Valves: Typically ring shaped over the region of the heart.
Pacemaker: Typically found in the left upper chest as radio-opaque discs. Make note of how many leads you see from the PPM/AICD
Let’s Try It!
Now that you have learned a systematic approach to chest radiograph interpretation, lets go over some examples:
Example 1
Rotation – no
Inspiration – mildly hyperinflated but not grossly
Penetration – appropriate
Prior – No
Airway – Trachea, carina and right/left bronchi all medial and also patent
Breathing – Right lower lobe opacification, airway markings bilaterally to chest wall
Cardiac – not enlarged, right and left cardiac borders not obscured
Diaphragm – sharp bilateral costophrenic angles, right diaphragm a bit obscured by air
bronchograms. Some increased lucency under left diaphragm correlating with gastric bubble
Everything else – Aortic knuckle and window also appropriate, no fractures, bilateral breast tissue symmetrical, no heart valves or lines noted
Diagnosis: RLL consolidation. Without history this would likely be diagnosed as a RLL Pneumonia
EXAMPLE 2

This is a 40 y/o M who presented to your urgent care with a 1 month history of increased SOB, dry cough and fatigue. He has also noted a 10 lbs weight gain in the last 2 weeks and bilateral lower extremity edema.
Rotation – not rotated
Inspiration – Good inspiration
Penetration – appropriate
Prior – none
Airway – Trachea and bilateral mainstem bronchi visible, midline and patent
Breathing – Complete opacification of the right lower lung with meniscus sign, air markings to chest wall bilaterally
Cardiac – right cardiac border is obscured so difficult to fully ascertain the size of the heart but does not seem overly enlarged
Diaphragm – sharp left costophrenic angle, right diaphragm and costophrenic angle obliterated and meniscus sign also noted
Everything Else – Aortic knuckle and window noted, no bone or soft tissue abnormalities, no lines/valves or PPM
Diagnoses: Right pleural effusion, likely related to CHF but further diagnostics required for that conclusion to be confirmed.
EXAMPLE 3
Go through R.I.P and A.B.C.D.E on your own. What do you see?

This patient is a 66 y/o F s/p median sternotomy (see those sternal wires) and MVR, AVR. Did you miss that there were also two valves? The MVR tends to lay more en-face so the actual diameter of the valve is easier to assess. The AVR lays more medially over the spine.
EXAMPLE 4

What do you see? STOP, go through your evaluation before moving on!
What if I told you that this patient is 55 y/o and presented to the emergency room with SOB after slipping on ice and falling on their right side? Does that change your findings?
Diagnosis: This patient has a traumatic right pneumothorax also with fractures of the right 3-8 ribs and displacement of the 5th and 6th ribs. There is also subcutaneous emphysema of the right chest wall.
Did you find this article helpful? If so, check out our Skills and Procedure Workshop!